
It has been touted as the modern alternative to a surgery thousands of people undergo around the world every year. A hip new technology which has seen dedicated websites with catchy names like ‘surfacehippy’ being established to promote its successes.
But as thousands more people prepare to undergo the new hip-resurfacing surgery, researchers in the US and UK are urging caution following studies which suggest the procedure is not ideal for everyone.
Go deeper with GlobalData

Discover B2B Marketing That Performs
Combine business intelligence and editorial excellence to reach engaged professionals across 36 leading media platforms.
Hip resurfacing has gained a lot of momentum in recent years, particularly in the US where manufacturer Smith & Nephew was given FDA approval in May 2006 for the launch of its proprietary Birmingham hip-resurfacing system. This was then followed in 2007 by interest from orthopaedic device company Stryker which was soon granted a ten-year distribution agreement for British company, Corin Group’s, Cormet hip-resurfacing system.
But now studies on both sides of the pond have issued words of concern. The Royal College of Surgeons in London and the Rush University Medical Center in Chicago both conducted studies completed within the autumn of 2008 and found that a patient’s age and gender are keys to the operation’s success.
The studies suggest that in many cases, total hip replacement is still the most successful procedure.
Surface results

US Tariffs are shifting - will you react or anticipate?
Don’t let policy changes catch you off guard. Stay proactive with real-time data and expert analysis.
By GlobalDataHip resurfacing, introduced in the late 1990s, is the alternative to the more conventional total hip replacement. It is aimed at middle-aged patients who are physically active and expected to outlive the normal lifespan of a full hip replacement which is usually 15 to 20 years. In addition, supporters say that because the procedure maintains more of the patient’s own thigh bone than conventional methods, patients are better able to tolerate complete replacement surgery later on in life.
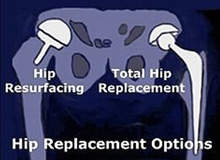
In a conventional total hip replacement orthopaedic surgeons remove the head of the femur, or the ball of the hip joint, and replace it with a metal stem inserted into the thigh bone. They fit the socket of the joint with a metal shell that typically includes a plastic liner.
In hip resurfacing the femoral head remains, but its surface is reshaped to accept a rounded cap with a short stem that sits in the femur. A thin metal cup is then pressed into the hip socket. Both components are made entirely of the metal cobalt chrome.
However, the British study by The Royal College of Surgeons published this September in the open-access journal PLoS Medicine, found 3.7% of the 2,360 women who underwent resurfacing in England had to have a second operation to repair the same hip within three years. Those women who received traditional hip replacements had a reoperation rate of 1.6% or less.
The study looked at traditional hip replacements, hip resurfacing and unicondylar knee surgery (where only half of the knee joint is replaced) and found in the UK about one in 75 patients had to undergo revision to their surgery within the first three years of total hip replacement or knee surgery, while the number was greater still in those who underwent hip resurfacing and more likely in women.
Nearly 170,000 procedures between 2003 and 2006 were analysed and in total there was a revision rate of 0.9% in total hip replacement, cemented to the bone, while hip resurfacing had a revision rate of 2.6%.
“Further research over longer timescales is needed to find out if this variation persists, why, and narrow down which patients would most benefit from these operations,” the report stated.
The figures however were still lower than other countries that run joint registries, Norway, Australia and Sweden, which all reported higher rates.
Jan van der Meulen, of the London School of Hygiene and Tropical Medicine, who led the study, says: “On the basis of our data, consideration should be given to using hip resurfacing only in male [patients].”
A recommendation was also made for a national registry to be established to better track the technology. John Black, president of the Royal College of Surgeons says; “By having a national registry and linking with routinely collected patient data we can quickly evaluate these technical innovations and ensure patients get the best possible outcomes from their surgery, even better than they are at the moment.”
Patient suitability
Research from the US found the majority of complications with hip resurfacing occurred in women of all ages and men over the age of 55. The study published online and due to appear in the journal Clinical Orthopaedics and Related Research in January 2009, reviewed 537 surgeries performed in the US using the Smith & Newman’s hip-resurfacing device, the first approved by the FDA.
“The ideal patients for hip resurfacing are males under the age of 55. They have the fewest, and the least serious, complications,” says Dr Craig Della Valle, lead author and a specialist in joint reconstruction at Rush University Medical Center.
The most common complication was a fracture of the femoral neck, the area of bone just beneath the head of the femur. “Patients may be eager to take advantage of technological innovations, but for older individuals, a conventional hip replacement is generally more appropriate,” Della Valle says.
The study found serious complications occurred in 32 of the 537 cases, including ten cases in which the femoral neck fractured after surgery. “Nine of the fractures in the study occurred in patients who were either female or older than 55 at the time of the implant. Eight of the fractures occurred when the surgeon was relatively inexperienced with the procedure [within the surgeon’s first ten cases],” the study said.
“Patients who are older or who are female tend to have softer bone,” Della Valle added. “Also, men on average have larger bone structures, with a greater surface area for securing the implant.”
Dr Peter Heekt, the chief medical officer of Smith & Nephew’s orthopaedic division said in a recent interview the company had advised resurfacing should not be used in older women or those with poor bone quality.
Unknown territory
Experts say hip resurfacing is more difficult to perform than traditional hip replacement because of the delicate reshaping of the top of the femur. A Smith & Nephew spokesman also recently said he thought the size of a candidates’ femur was a better indicator if resurfacing would suit a patient. But experts acknowledge there is no conclusive test to determine who will be the best candidate for resurfacing and there have been reports in the US of some surgeons refusing to perform the surgery irrespective of the candidate.
In the US during 2006 resurfacing represented a small fraction of the 430,000 hip replacements that took place – roughly about 15,000. However, that number is expected to grow by between 40% and 50% in the near future. While in the UK, hip and knee surgeries are among one of the most common operations with around 160,000 carried out in England and Wales in 2006.
As the concerns grow the FDA has now asked both Smith & Nephew and Stryker to perform studies of patient outcomes. But others, such as Della Valle, still insist it has its advantages. “It preserves more bone because the head of the femur is retained. It enables the patient to return to high-impact sports because the metal components of the implant resist wear and tear and can withstand the forces associated with activities like running. Some studies have also shown that hip resurfacing carries a lower risk of dislocation because the size of the ball component is larger.”
But despite its benefits, risks remain and even those in the business add the clarifier of ‘this is not for everyone’.

